Ai Overview
A HIPAA compliant blockchain architecture requires deliberate design choices that balance distributed ledger transparency with strict healthcare privacy regulations. Achieving compliance demands specific consensus mechanisms, node governance structures, and cryptographic frameworks that satisfy the Security Rule’s technical safeguards and the Privacy Rule’s minimum necessary standard.
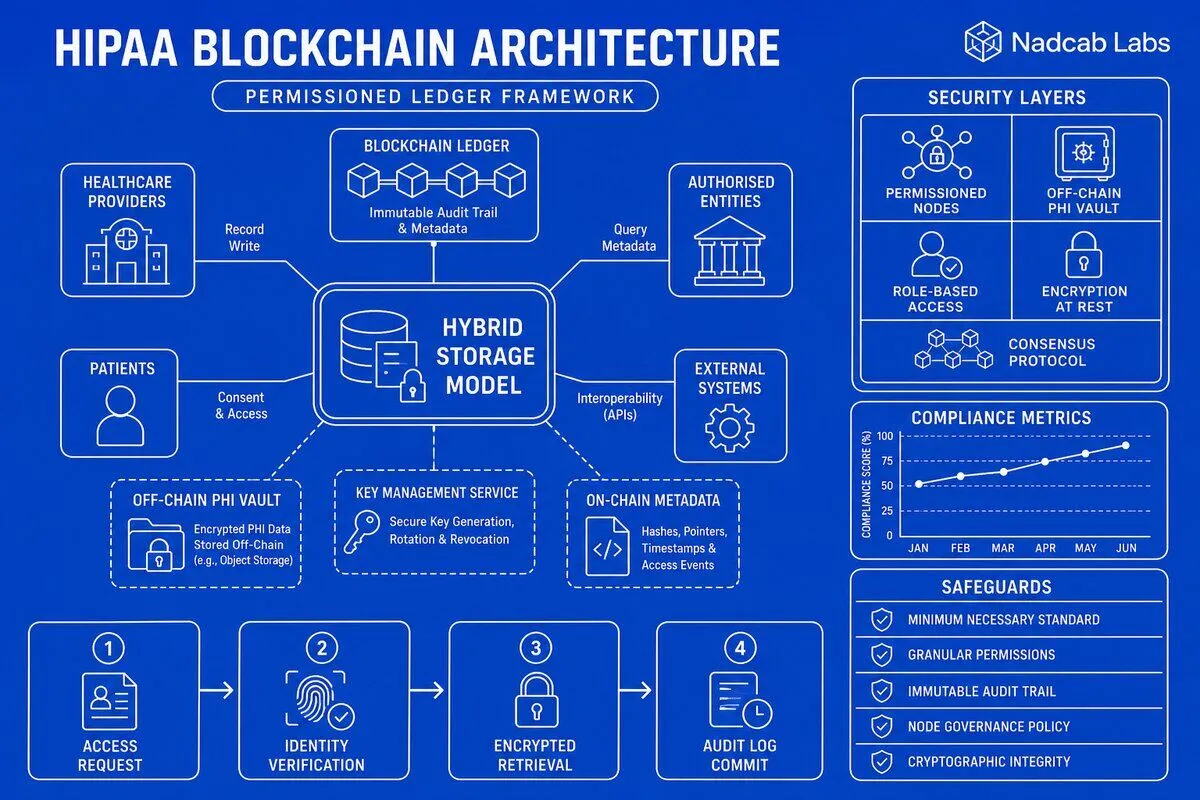
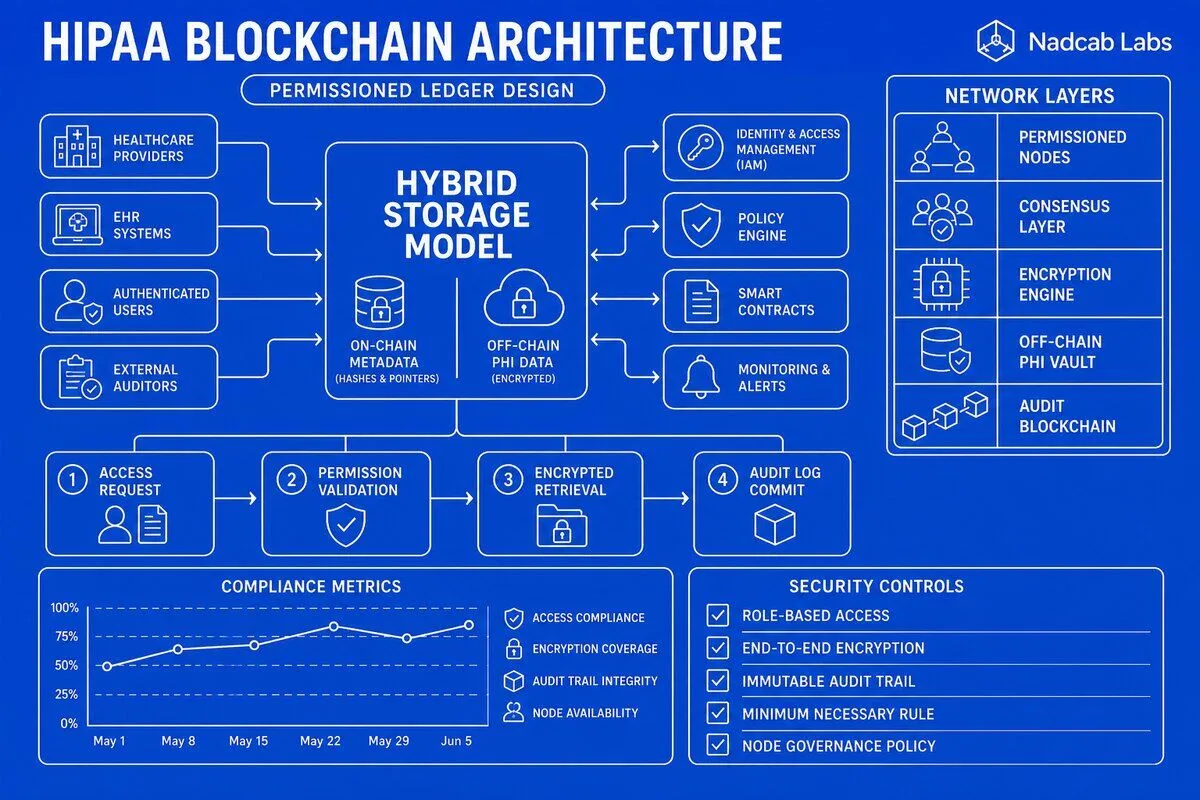
A HIPAA compliant blockchain architecture requires deliberate design choices that balance distributed ledger transparency with strict healthcare privacy regulations. Unlike public blockchains where all transaction data is visible to every network participant, healthcare systems must implement permissioned networks with layered encryption, granular access controls, and off-chain storage patterns that protect Protected Health Information (PHI) while maintaining audit integrity. Achieving compliance demands specific consensus mechanisms, node governance structures, and cryptographic frameworks that satisfy the Security Rule’s technical safeguards and the Privacy Rule’s minimum necessary standard.
Key Takeaways
- Public blockchains violate HIPAA by default due to immutable PHI exposure; permissioned architectures with role-based access are mandatory
- Hybrid on-chain/off-chain patterns store only metadata and audit logs on-chain while keeping encrypted PHI in separate secure databases
- PBFT and RAFT consensus mechanisms paired with Business Associate Agreement-bound node operators satisfy HIPAA security requirements
- Multi-layer encryption (AES-256 at rest, TLS 1.3 in transit, attribute-based for granular consent) prevents unauthorized PHI disclosure
- Smart contracts automate consent tracking, audit trail generation, and breach notification while maintaining immutable compliance records
- Patient-controlled private keys with hierarchical deterministic key management enable self-sovereign identity and provider delegation
What makes blockchain architecture HIPAA compliant by default versus requiring custom design?
Standard public blockchain architectures fundamentally conflict with HIPAA regulations because they prioritize transparency and immutability over privacy. Every transaction on networks like Ethereum or Bitcoin is visible to all participants and permanently recorded, meaning any PHI written to the chain becomes publicly accessible forever. The HIPAA Privacy Rule explicitly prohibits such broad disclosure, requiring that only the minimum necessary information be shared with authorized entities for specific purposes. Public blockchains also lack mechanisms to enforce the Security Rule’s administrative, physical, and technical safeguards, making them unsuitable for healthcare data without substantial modification.
Permissioned blockchain networks address these violations by implementing identity-verified node operators and role-based access control at the protocol level. In a permissioned architecture, only pre-approved entities—hospitals, insurers, pharmacy systems—can join the network, and each participant receives specific read/write permissions tied to their role. This structure mirrors the HIPAA concept of Covered Entities and Business Associates, where every party handling PHI must sign agreements and implement required safeguards. Our healthcare software development team designs these permission layers to enforce the minimum necessary standard automatically, ensuring that a billing department cannot access clinical notes and a pharmacy cannot view insurance claims unrelated to prescription fulfillment.
The immutability property of blockchain also requires careful architectural consideration. HIPAA grants patients the right to amend inaccurate records, which seems incompatible with a ledger where data cannot be deleted or altered. Compliant architectures solve this through versioning patterns: the blockchain stores cryptographic hashes and access logs rather than actual PHI, while the mutable medical records reside in traditional encrypted databases. When a patient requests an amendment, the off-chain database updates the record, and the blockchain records a new hash pointer with a timestamp and justification. This preserves an immutable audit trail of who changed what and when, satisfying both HIPAA’s amendment rights and the Security Rule’s requirement for integrity controls.
Default blockchain consensus mechanisms also fail HIPAA’s availability requirements. Proof-of-work networks can experience significant latency and are vulnerable to 51% attacks if a single entity controls the majority of mining power. Healthcare systems need guaranteed uptime and Byzantine fault tolerance to ensure that emergency room physicians can access critical patient data even if some network nodes are offline or compromised. Compliant architectures therefore require custom consensus protocols like Practical Byzantine Fault Tolerance (PBFT) or RAFT, which provide fast finality and tolerate up to one-third of nodes behaving maliciously or failing. These mechanisms are paired with service level agreements that specify maximum downtime thresholds, aligning technical architecture with HIPAA’s contingency planning requirements.
How do you architect hybrid on-chain/off-chain storage for protected health information?
The hybrid storage pattern separates metadata and access control logic (stored on-chain) from the actual PHI (stored off-chain in encrypted databases). On the blockchain, you record cryptographic hashes of medical documents, patient consent states, and audit logs of every access event. Off-chain, you maintain the full medical records in HIPAA-compliant databases with encryption at rest using AES-256 and strict access controls. When a provider needs to view a patient’s lab results, the smart contract verifies their authorization on-chain, then returns a decryption key that allows the provider’s system to retrieve and decrypt the specific document from the off-chain storage. This architecture ensures that even if the blockchain is compromised, attackers gain no access to readable PHI—only hashes and access logs.
Cryptographic hash pointers create an immutable link between the on-chain ledger and off-chain data stores. Each time a new medical record is created, the system generates a SHA-256 hash of the encrypted document and writes that hash to the blockchain along with metadata like document type, creation timestamp, and the patient’s public key identifier. The hash serves as a tamper-evident seal: if anyone modifies the off-chain document, the recalculated hash will not match the blockchain record, immediately revealing the integrity violation. This pattern is similar to private blockchain architecture design patterns used in financial systems, but adapted for healthcare’s stricter confidentiality requirements.
Data segregation strategies ensure that only authorized entities can decrypt and access sensitive records. One effective pattern uses attribute-based encryption (ABE), where each medical record is encrypted with a policy specifying required attributes—for example, “cardiologist” AND “treating_physician” AND “patient_consent_active”. Only users whose credentials satisfy all attributes can decrypt the record. The blockchain stores the encrypted data location and access policy, while the key management system verifies attributes before issuing decryption keys. This granular control satisfies HIPAA’s minimum necessary standard by preventing over-broad access: a billing clerk cannot decrypt clinical notes even if they gain access to the off-chain storage system, because their role attributes do not match the encryption policy.
The following table compares storage approaches for different types of healthcare data in a compliant architecture:
| Data Type | Storage Location | Encryption Method | Access Control |
|---|---|---|---|
| Patient consent records | On-chain (smart contract state) | None (public metadata only) | Patient-signed transactions |
| Clinical notes and diagnoses | Off-chain encrypted database | AES-256 + ABE | Role + consent verification |
| Medical imaging (X-rays, MRIs) | Off-chain HIPAA-compliant cloud storage | AES-256 + patient-specific keys | Time-limited access tokens |
| Access audit logs | On-chain (event logs) | None (non-PHI metadata) | Immutable, public to authorized auditors |
| Document hashes and pointers | On-chain (transaction data) | SHA-256 hash only | Read access for all network participants |
| Prescription records | Hybrid (summary on-chain, details off-chain) | Partial encryption (drug name encrypted off-chain) | Provider + pharmacy + patient access |
Emergency access override protocols are critical for life-threatening situations where normal consent workflows would delay treatment. The architecture includes a “break-glass” mechanism: an emergency room physician can invoke a special smart contract function that grants temporary access to a patient’s critical records (allergies, current medications, blood type) without prior consent. Every break-glass access is logged on-chain with the physician’s identity, timestamp, and justification. Hospital compliance officers review these logs weekly to detect abuse, and patients receive automatic notifications when their records are accessed under emergency provisions. This balances HIPAA’s treatment exception with the Security Rule’s requirement for accountability.
Which consensus mechanisms and node configurations satisfy HIPAA security rules?
Practical Byzantine Fault Tolerance (PBFT) consensus provides the deterministic finality and low latency required for healthcare applications. In a PBFT network, transactions are confirmed when two-thirds of validator nodes agree on the ordering and validity of each block. This means a network with 10 validators can tolerate up to 3 malicious or offline nodes while maintaining integrity and availability. PBFT achieves finality in seconds rather than the minutes or hours required by proof-of-work, ensuring that when a physician submits a prescription, it is irreversibly recorded before the patient leaves the office. The protocol’s formal mathematical proofs of correctness align with HIPAA’s requirement for data integrity controls that detect unauthorized alterations.
RAFT consensus offers a simpler alternative for smaller healthcare networks where Byzantine fault tolerance is less critical. RAFT elects a leader node that coordinates transaction ordering, with follower nodes replicating the leader’s log. If the leader fails, followers automatically elect a new leader within milliseconds. This architecture works well for regional health information exchanges where all participating hospitals have established trust relationships and signed Business Associate Agreements. RAFT’s simplicity reduces the attack surface compared to more complex consensus protocols, making security audits and HIPAA compliance assessments more straightforward. However, RAFT only tolerates crash failures, not malicious behavior, so it requires strong perimeter security and intrusion detection systems.
Proof-of-authority (PoA) consensus assigns validation rights to a fixed set of approved entities—typically major healthcare institutions, government health agencies, or established health IT vendors. Each validator stakes their reputation and legal liability rather than computational power or tokens. Validators sign each block with their private key, creating a clear chain of accountability: if a block contains fraudulent transactions, auditors can identify exactly which validator approved it. This accountability mechanism satisfies HIPAA’s requirement that Covered Entities and Business Associates be legally responsible for safeguarding PHI. PoA networks typically run with 15-25 validators to balance decentralization with performance, processing 500-1000 transactions per second with sub-second finality.
Node operator requirements must include Business Associate Agreements that explicitly define each validator’s HIPAA obligations. The agreement specifies technical safeguards the operator must implement: encrypted storage, regular security audits, incident response procedures, and breach notification timelines. Operators must also undergo annual compliance assessments and provide evidence of workforce training on PHI handling. These contractual and technical requirements transform blockchain validators from anonymous network participants into legally accountable healthcare entities. When designing node configurations, architects must consider geographic distribution to prevent regional outages while ensuring all nodes reside in jurisdictions with strong data protection laws—typically avoiding countries without adequate privacy regulations.
The following process flow illustrates how a healthcare transaction achieves consensus in a PBFT-based HIPAA compliant network:
Validator authentication protocols ensure that only authorized nodes participate in consensus. Each validator possesses a hardware security module (HSM) storing their private signing key, which never leaves the device. When joining the network, validators must present a certificate signed by the network’s governance authority—typically a healthcare consortium or government health agency. The certificate includes the validator’s legal entity information, Business Associate Agreement reference number, and allowed transaction types. Smart contracts verify this certificate before accepting any blocks signed by that validator. This multi-layer authentication prevents rogue actors from injecting malicious nodes into the network, a critical safeguard given that healthcare data breaches can expose millions of patient records.
Byzantine fault tolerance thresholds must account for the healthcare industry’s concentration risk. If three major hospital systems operate 60% of the network’s validators, a coordinated attack or simultaneous system failure could compromise consensus. Architects address this by setting governance rules that limit any single organization to controlling no more than 20% of validators, and requiring geographic distribution across at least three regions. The network should maintain at least 10 active validators at all times, ensuring that even if 3 validators fail simultaneously, the remaining 7 can still achieve the two-thirds majority required for PBFT consensus. These thresholds are documented in the network’s governance charter and enforced through smart contract logic that rejects new validator registrations that would violate concentration limits.
What encryption and key management architecture prevents unauthorized PHI disclosure?
Multi-layer encryption protects PHI throughout its lifecycle in a blockchain healthcare system. At rest, all off-chain databases use AES-256 encryption with keys stored in FIPS 140-2 Level 3 certified hardware security modules. These HSMs ensure that even database administrators cannot access decryption keys without multi-party authorization. In transit, all network communications use TLS 1.3 with perfect forward secrecy, meaning that even if an attacker records encrypted traffic and later compromises a server’s private key, they cannot decrypt past sessions. At the smart contract level, sensitive data fields within transactions are encrypted using the recipient’s public key before being submitted to the blockchain, ensuring that only the intended recipient can decrypt the information even though the transaction itself is visible to all validators.
Hierarchical deterministic (HD) key management provides a scalable structure for managing thousands of encryption keys across a healthcare network. The architecture starts with a master seed controlled by the patient, from which all subsidiary keys are mathematically derived. A patient’s master key generates separate child keys for different purposes: one for primary care records, another for specialist visits, another for pharmacy records. Each child key can further generate grandchild keys for specific providers or time periods. This hierarchy means patients can delegate access to a specialist by sharing a derived key that only unlocks cardiology records from the past six months, without exposing their entire medical history. The derivation paths are recorded on-chain, creating an auditable trail of which keys were generated and for what purpose.
Patient-controlled private keys shift the security model from institution-centric to patient-centric, aligning with HIPAA’s individual rights provisions. Each patient generates a key pair during enrollment, with the private key stored on their smartphone or hardware wallet. When a provider needs access, the patient’s app displays a consent request showing exactly what data will be shared and for how long. The patient approves by signing a transaction with their private key, which updates the on-chain consent registry. This architecture eliminates the risk of mass data breaches that occur when centralized hospital databases are compromised—an attacker would need to compromise each patient’s individual device rather than a single database containing millions of records. The tradeoff is that patients must securely backup their keys, typically using multi-party computation schemes that split the key across the patient’s devices and trusted recovery partners.
Provider delegation mechanisms allow patients to grant temporary access without sharing their master private key. Using proxy re-encryption, a patient can authorize a smart contract to transform data encrypted with the patient’s public key into data encrypted with the provider’s public key, without the smart contract ever seeing the plaintext data. For example, when a patient schedules surgery, they delegate access to the surgical team for a 30-day window. The smart contract automatically re-encrypts relevant medical records so the surgical team can decrypt them using their own keys. After 30 days, the delegation expires and the surgical team can no longer decrypt the records, even if they saved the encrypted data. This time-bounded access satisfies HIPAA’s minimum necessary standard by ensuring providers only access PHI for the duration of active treatment.
Attribute-based encryption (ABE) enables fine-grained access control based on provider roles and patient consent. Each medical record is encrypted with a policy expressed as a boolean formula—for example, “(role=physician AND specialty=cardiology AND patient_consent=active) OR (role=emergency_physician AND emergency_override=true)”. The key authority issues private keys to providers that contain cryptographic attributes corresponding to their verified credentials. A cardiologist receives a key embedded with the attributes “role=physician” and “specialty=cardiology”, while an emergency room physician receives a key with “role=emergency_physician”. Only when a provider’s key attributes satisfy the encryption policy can they decrypt the record. This cryptographic enforcement of access control policies is more secure than traditional database access controls, which can be bypassed by privileged administrators or SQL injection attacks.
Emergency access override protocols use threshold cryptography to enable life-saving access without compromising routine security. The patient’s master key is split into five shares using Shamir’s Secret Sharing, with any three shares sufficient to reconstruct the key. The patient holds two shares, their primary care physician holds one, a trusted family member holds one, and the hospital’s ethics committee holds one. In an emergency where the patient is unconscious, the emergency physician, primary care physician, and ethics committee can combine their shares to temporarily reconstruct the patient’s key and access critical medical information. Every emergency access event is logged on-chain with justifications, and patients are notified once they regain consciousness. This mechanism balances HIPAA’s treatment exception with accountability requirements.
The following bar chart shows the relative security strength of different encryption approaches in healthcare blockchain systems:
Encryption Method Security Comparison (Higher = Stronger)
Key rotation policies ensure that even if a key is compromised, the window of exposure is limited. The architecture automatically rotates encryption keys every 90 days, re-encrypting all affected data with new keys. The old keys are archived in the HSM for a retention period (typically seven years to match HIPAA record retention requirements), allowing authorized parties to decrypt historical records if needed for audits or legal proceedings. The blockchain records each key rotation event with timestamps and the hash of the new public key, creating an immutable audit trail. This rotation schedule satisfies HIPAA’s requirement for periodic security reviews and updates to safeguards as technology and threats evolve.
How do smart contracts enforce patient consent and audit logging for HIPAA compliance?
Consent management smart contracts create an immutable registry of patient authorization decisions that automatically enforce access control policies. When a patient grants consent for a specific provider to access their records, the patient signs a transaction that invokes the consent contract’s “grantAccess” function with parameters specifying the provider’s identity, data categories (lab results, prescriptions, clinical notes), purpose (treatment, payment, operations), and expiration date. The contract emits an event logging this consent grant with a timestamp, and updates its internal state to reflect the new authorization. Every subsequent attempt to access the patient’s data must first query the consent contract to verify that active, unexpired consent exists for that specific provider and data category. If the query returns false, the access request is automatically denied before any PHI is retrieved.
The consent contract architecture supports granular permissions that go beyond simple yes/no authorization. Patients can specify that their cardiologist can view cardiovascular records but not psychiatric records, or that their insurer can access billing codes but not clinical notes. These rules are encoded as a permission matrix within the contract’s storage, with each cell representing a specific (provider, data category, purpose) tuple and its allowed/denied status. When implementing these contracts, developers must carefully optimize gas costs, as storing large permission matrices on-chain can become expensive. A common pattern is to store only exceptions to default rules on-chain: if the patient has not explicitly restricted access, the default HIPAA minimum necessary standard applies, but any specific grants or denials override the default.
Consent revocation mechanisms allow patients to withdraw authorization at any time, as required by HIPAA. The patient invokes the contract’s “revokeAccess” function, which immediately updates the permission registry and emits a revocation event. Crucially, the contract does not delete the original consent grant record—that would violate the audit trail requirement. Instead, it appends a revocation record with a timestamp, creating a complete history of the patient’s consent decisions. Providers’ systems listen for these revocation events and must immediately cease accessing the patient’s data. The smart contract can enforce this by integrating with the key management system to invalidate the provider’s decryption keys for that patient’s records within seconds of revocation. This rapid propagation of consent changes is only possible with blockchain’s real-time event notification capabilities.
Automated audit trail generation captures every PHI access event without requiring manual logging by providers. Each time a provider’s system requests access to patient data, it must call the consent contract’s “logAccess” function, passing parameters that identify the provider, patient, data accessed, timestamp, and purpose. The contract verifies that consent exists, then emits an “AccessLogged” event that is permanently recorded in the blockchain’s transaction log. These events form an immutable, tamper-proof audit trail that satisfies HIPAA’s requirement for tracking disclosures of PHI. Unlike traditional audit logs stored in mutable databases where a malicious administrator could delete entries, blockchain-based logs cannot be altered after the block is finalized. Compliance officers can query these logs to generate reports showing all accesses to a patient’s records over any time period, with cryptographic proof that the logs are complete and unmodified.
The audit contract also tracks metadata about each access event that HIPAA requires: the identity of the person or entity receiving the PHI, the date of disclosure, a description of the PHI disclosed, and the purpose of the disclosure. For automated disclosures (like a pharmacy system retrieving a prescription), the contract logs the system identifier and the API endpoint called. For manual accesses (like a physician viewing records through an EHR interface), the contract logs the physician’s credential identifier and workstation location. This granular tracking enables detection of suspicious patterns: if a physician who normally accesses 10 patient records per day suddenly accesses 500 records, the anomaly detection system flags this for investigation. Such behavioral analytics are only feasible with comprehensive, structured audit data that blockchain provides.
Breach notification triggers automate compliance with HIPAA’s 60-day breach notification rule. The smart contract monitors for events that indicate potential breaches: multiple failed access attempts from the same IP address, access to records for patients the provider has no treatment relationship with, or bulk data exports outside normal business hours. When the contract detects a suspicious pattern, it automatically emits a “PotentialBreach” event that triggers the organization’s incident response workflow. The contract can also enforce the notification timeline by tracking the date a breach was discovered and automatically escalating to senior compliance officers if a notification has not been filed within 58 days. This automation reduces the risk of missed deadlines that can result in substantial HIPAA penalties.
The following table details the smart contract functions required for comprehensive HIPAA compliance automation:
| Contract Function | Purpose | Key Parameters | HIPAA Requirement Satisfied |
|---|---|---|---|
| grantConsent() | Patient authorizes provider access | providerID, dataCategories[], purpose, expirationDate | Individual authorization (Privacy Rule §164.508) |
| revokeConsent() | Patient withdraws authorization | providerID, effectiveDate | Right to revoke authorization (Privacy Rule §164.508(b)(5)) |
| verifyAccess() | Check if access is permitted | providerID, patientID, dataCategory, purpose | Minimum necessary standard (Privacy Rule §164.502(b)) |
| logAccess() | Record PHI disclosure event | providerID, patientID, dataAccessed, timestamp, purpose | Accounting of disclosures (Privacy Rule §164.528) |
| requestAmendment() | Patient requests record correction | recordHash, amendmentText, justification | Right to amend (Privacy Rule §164.526) |
| emergencyOverride() | Break-glass access for emergencies | providerID, patientID, justification, witnessID | Treatment exception (Privacy Rule §164.506(c)) |
| reportBreach() | Log potential security incident | incidentType, affectedRecords, discoveryDate | Breach notification (Breach Notification Rule §164.404) |
| generateAccountingReport() | Compile disclosure history | patientID, startDate, endDate | Accounting of disclosures (Privacy Rule §164.528) |
Event-driven compliance reporting uses smart contract events to automatically generate the reports HIPAA requires. When a patient requests an accounting of disclosures, the system queries the blockchain for all “AccessLogged” events associated with that patient’s identifier over the requested time period. The contract aggregates these events into a structured report showing the date of each disclosure, the recipient, the information disclosed, and the purpose. This report generation is instantaneous and cryptographically verifiable—the patient can independently verify that the report is complete by querying the blockchain themselves. Traditional manual accounting processes can take weeks and are prone to omissions; blockchain automation reduces this to seconds with guaranteed completeness.
Smart contract integration with existing healthcare IT systems requires careful API design to bridge on-chain and off-chain worlds. Electronic Health Record (EHR) systems call the blockchain’s RPC endpoints to invoke consent contract functions, passing patient and provider identifiers that map to on-chain addresses. The blockchain returns authorization decisions that the EHR enforces before displaying PHI. This architecture is similar to patterns used in blockchain KYC AML compliance architecture, where external systems query smart contracts to verify identity and authorization. The key difference is that healthcare systems must handle HIPAA’s stricter requirements for audit trails and patient rights. Middleware layers often implement caching to reduce blockchain query latency, storing recent consent decisions locally but refreshing them every few minutes to catch revocations.
The consent contract architecture also supports delegation chains for complex healthcare scenarios. A patient might authorize their primary care physician, who then delegates access to a specialist, who delegates to a laboratory for test interpretation. Each delegation is recorded as a separate consent grant on-chain, creating a traceable chain from the patient’s original authorization to the final data access. This satisfies HIPAA’s requirement that Covered Entities document the chain of custody for PHI. The smart contract enforces that delegations cannot grant more permissions than the delegator possesses—if the primary care physician only has access to cardiovascular records, they cannot delegate access to psychiatric records. This hierarchical permission model mirrors real-world clinical workflows while maintaining cryptographic enforcement of the minimum necessary principle.
Integration with token vesting smart contract architecture patterns enables innovative payment models tied to compliance. Healthcare organizations can receive token incentives for maintaining high compliance scores measured by smart contract metrics: percentage of accesses with valid consent, average audit log completeness, breach notification response time. These tokens vest over time as the organization demonstrates sustained compliance, creating financial incentives for HIPAA adherence. The vesting contract automatically tracks compliance metrics by querying the consent and audit contracts, and releases tokens when thresholds are met. This gamification of compliance can be particularly effective for smaller healthcare providers who lack dedicated compliance departments.
Consent contracts also facilitate patient-mediated data exchange, where patients control which providers can share information with each other. Traditional health information exchanges require providers to establish bilateral agreements, creating a complex web of relationships. With blockchain-based consent, the patient grants access to multiple providers and specifies whether each provider can see what the others are doing. For example, a patient might allow their cardiologist and endocrinologist to both view the patient’s full record and see each other’s notes, but prevent their psychiatrist’s notes from being visible to other specialists. These nuanced sharing rules are encoded in the consent contract’s permission matrix and enforced automatically, giving patients true control over their health information as HIPAA envisions.
The architecture must also address HIPAA’s requirement for consent to be “written” and “signed” by the patient. In a blockchain context, a patient’s digital signature on a transaction serves as the legal equivalent of a written signature, provided the system uses strong cryptographic signatures (ECDSA or EdDSA) and the patient’s identity has been verified through a Know Your Customer (KYC) process. The consent contract stores the hash of the consent form text along with the patient’s signature, proving that the patient agreed to specific terms. This approach has been validated in legal contexts through frameworks like eIDAS in Europe and ESIGN in the United States, which recognize digital signatures as legally binding. Healthcare organizations implementing this architecture should consult legal counsel to ensure their jurisdiction recognizes blockchain-based consent as HIPAA-compliant.
Our modular blockchain solutions enable healthcare organizations to adopt these consent and audit capabilities incrementally. Rather than replacing entire EHR systems, organizations can deploy a consent management layer that sits between existing systems and data stores. This layer intercepts all data access requests, verifies permissions against the blockchain consent registry, logs the access on-chain, then proxies the request to the legacy system if authorized. This modular approach reduces implementation risk and allows organizations to prove compliance benefits before committing to full blockchain migration. The consent layer can also integrate with Blockchain Identity Management systems to provide unified authentication across multiple healthcare providers, creating a seamless patient experience while maintaining strict access controls.
Finally, the smart contract architecture must support HIPAA’s requirements for Business Associate subcontractor management. When a Covered Entity uses a cloud storage provider to host off-chain PHI, that provider is a Business Associate and must sign a BAA. The blockchain records the hash of each BAA along with its effective and expiration dates. The consent contract verifies that a valid BAA exists before allowing any entity to access encryption keys or off-chain data. If a BAA expires without renewal, the contract automatically revokes that entity’s access privileges, preventing unauthorized PHI disclosure. This automated BAA management reduces the compliance burden on healthcare organizations and ensures that the chain of legal accountability remains intact even as subcontractor relationships change over time.
The combination of consent management, audit logging, and automated compliance reporting creates a comprehensive HIPAA-compliant architecture that surpasses traditional database-centric approaches in transparency, accountability, and patient control. By encoding regulatory requirements as executable smart contract logic, healthcare organizations shift from manual compliance processes that are error-prone and audit-intensive to automated systems that provide continuous compliance assurance. This architectural shift is particularly valuable as healthcare moves toward value-based care models that require extensive data sharing across organizational boundaries—blockchain provides the trust infrastructure that makes such sharing possible while protecting patient privacy.
Organizations building these systems should also consider how the architecture integrates with emerging technologies. Machine Learning Architecture for clinical decision support can query the consent contract to ensure that patient data used for model training has appropriate authorization. Web3 Architecture patterns enable patients to monetize their health data by granting pharmaceutical researchers access in exchange for tokens, with all transactions governed by smart contracts that enforce HIPAA’s research authorization requirements. These integrations demonstrate that HIPAA compliant blockchain architecture is not just about regulatory compliance—it’s a foundation for innovative healthcare business models that were impossible with centralized data systems.
Final Thoughts
Building a HIPAA compliant blockchain architecture requires systematic attention to permissioned network design, hybrid storage patterns, consensus mechanisms with legal accountability, multi-layer encryption with patient-controlled keys, and smart contracts that automate consent and audit requirements. The architecture must balance blockchain’s transparency and immutability with healthcare’s strict privacy mandates, using techniques like off-chain PHI storage, attribute-based encryption, and granular access controls. Organizations that implement these patterns gain not only regulatory compliance but also enhanced patient trust, reduced breach risk, and the foundation for innovative data-sharing models. As healthcare continues its digital transformation, blockchain architectures that properly address HIPAA requirements will become essential infrastructure for secure, patient-centric care delivery. The technical complexity is significant, but the payoff—tamper-proof audit trails, automated compliance, and true patient data sovereignty—justifies the investment for any healthcare organization serious about protecting patient privacy while enabling modern clinical workflows.
Frequently Asked Questions
Q1.Is blockchain HIPAA compliant?
Blockchain technology itself is neither compliant nor non-compliant; HIPAA compliance depends on implementation. A properly architected permissioned blockchain with encrypted PHI, access controls, audit logs, BAAs with all chain participants, and administrative safeguards can meet HIPAA requirements. Public blockchains storing unencrypted health data violate HIPAA. Nadcab Labs designs enterprise healthcare blockchains with built-in compliance frameworks including encryption at rest and in transit, role-based permissions, and comprehensive audit trails.
Q2.What is the blockchain architecture in healthcare?
Healthcare blockchain architecture typically uses permissioned networks (Hyperledger Fabric, Quorum, or private Ethereum) with encrypted data storage, identity management layers, smart contract engines for consent and access logic, off-chain secure databases for large files, and API gateways connecting legacy EHR systems. Architecture includes cryptographic key management, multi-signature authorization, immutable audit trails, and disaster recovery mechanisms. Nadcab Labs implements modular designs separating PHI storage from transaction ledgers to balance transparency with privacy.
Q3.How does permissioned blockchain differ from public blockchain for healthcare data?
Permissioned blockchains restrict network participation to verified entities through identity management, enabling HIPAA-required access controls and BAAs. They offer configurable privacy (private channels, zero-knowledge proofs), faster consensus without mining, and governance aligned with healthcare regulations. Public blockchains lack access restrictions, expose all data to anonymous nodes, and cannot guarantee HIPAA compliance. Nadcab Labs exclusively deploys permissioned architectures for healthcare, using Hyperledger Fabric or enterprise Ethereum with private transactions and controlled validator sets.
Q4.What encryption standards are required for HIPAA compliant blockchain systems?
HIPAA mandates encryption meeting NIST standards: AES-256 for data at rest, TLS 1.2+ for data in transit, and SHA-256 or stronger for hashing. Blockchain implementations must encrypt PHI before chain storage, use hardware security modules (HSMs) for key management, implement secure key rotation, and maintain encrypted backups. Nadcab Labs integrates FIPS 140-2 validated cryptographic modules, multi-party computation for distributed key management, and zero-knowledge proofs enabling verification without exposing sensitive data.
Q5.Can smart contracts automatically enforce HIPAA patient consent requirements?
Yes, smart contracts can programmatically enforce HIPAA consent by encoding patient authorization rules, automatically verifying permissions before data access, logging all consent events immutably, and revoking access when consent expires or is withdrawn. Contracts check requester credentials, purpose of use, and time restrictions before releasing decryption keys or data pointers. Nadcab Labs develops consent management smart contracts with granular controls, emergency access override protocols, and real-time audit capabilities ensuring every data transaction has documented patient authorization.
Q6.How do you handle the HIPAA right to amend records on an immutable blockchain?
HIPAA amendment rights are addressed through append-only correction patterns: original records remain immutable but new transactions add amendments, corrections, or annotations with timestamps and provenance. Smart contracts display the current valid version while preserving complete history. Alternatively, store only hashes on-chain with actual PHI in amendable off-chain databases. Nadcab Labs implements versioned record systems where blockchain maintains an immutable audit trail of all amendments while presenting patients and providers with the legally current record version.
Explore Services
Related Services
Reviewed by

Wazid Khan
Director & Co-Founder
Wazid Khan is the Director & Co-Founder of Nadcab Labs, a forward-thinking digital engineering company specializing in Blockchain, Web3, AI, and enterprise software solutions. With a strong vision for innovation and scalable technology, Wazid has played a key role in building Nadcab Labs into a trusted global technology partner. His expertise lies in strategic planning, business development, and delivering client-centric solutions that drive real-world impact. Under his leadership, the company has successfully delivered numerous projects across industries such as fintech, healthcare, gaming, and logistics. Wazid is passionate about leveraging emerging technologies to create secure, efficient, and future-ready digital ecosystems for businesses worldwide.





